80% of the adult population will experience low back pain at some point in their life. Damage to the intervertebral discs, either through an acute injury or degenerative changes, can be a significant component of low back pain. However, a significant proportion of low back pain sufferers do not have a well-defined structural reason for their pain – we refer to this as non-specific back pain. Research has shown that plenty of people with healthy looking discs experience significant levels of pain and others with highly damaged discs experience no pain at all. This tells us that pain – which is the body’s warning system – has multiple origins and isn’t always directly linked to tissue damage. Pain and the experience of pain is deeply rooted in the interplay of anatomical, physiological, emotional, intellectual, experiential and sociological factors. For more information on pain, particularly chronic pain, read here
So what are our discs, what do they do and how does damage to them lead to pain and what can we do about it?
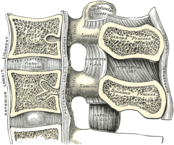
Our discs sit between our vertebrae within the spinal column and act to transmit and absorb loads through the body as we move. They also facilitate trunk and neck movement and create space for the spinal nerves to exit the spinal column and make their way to the rest of the body.
The discs have a fibrocartilaginous outer ring and a jelly-like core. Minor damage to the outer ring, known as the annulus, can lead to a bulging disc and in severe cases significant damage leads to a complete disc herniation. In these more severe cases the jelly-like core of the disc protrudes out from the annulus and compresses the spinal nerve roots leading to sciatica (insert hyperlink to sciatica) and other pain referral patterns.
Not all discogenic pain is due to direct nerve or tissue compression. Damage to the disc can alter the feedback pattern that the brain typically receives. Altered feedback leads to altered muscle recruitment causing changes in joint position leading to joint and tissue stress which is both a source of pain and a cause of muscle spasm and further pain.
When a disc is damaged the body releases a number of pro-inflammatory chemicals to deal with the injury. These chemicals can irritate our nerves contributing to our experience of pain.
Risk Factors / Causes:
Some people rupture their disc in response to a sudden increase in intradiscal pressure: for example during a heavy or high-speed lifting and/or twisting movement. In some cases this is literally the “straw that broke the camel’s back”, in that the load has caused failure in an already damaged or weakened disc wall. In others it is simply a load-induced failure of the disc.
Poor posture; poor core control; prolonged sitting and or trunk bending; inadequate work task rotation; and obesity all contribute to a higher risk profile for discogenic injury.
Management:
Most disc injuries can be managed successfully without the need for surgery. Some cases will proceed to surgery which may entail a stabilisation procedure; a discectomy or micro-discectomy: a procedure to remove herniated disc tissue impacting upon the nerve root; or even a disc replacement. Once the surgery has been performed we begin a process of rehabilitation that is very similar to what we undertake for the non-surgical patient: that is focusing on pain-management; re-education of movement patterns; improved core control; muscle strengthening and endurance training; and a return to full normal function.
Patients presenting with a disc injury often are in a lot of pain so we use techniques to reduce muscle spasm, support posture and reinforce pain-relieving movement patterns.
In addition to pain-management we look to restoring optimal joint movement; normalising muscle recruitment patterns; and enhancing core stability. All of these techniques are gradually progressed until we are replicating the loads that would be experienced in a work, leisure or sport environment. Many of our patients with discogenic pain respond well to Pilates-based exercise to improve their muscle strength and endurance and general joint and body mobility.
If you’re suffering from discogenic low back pain or would like to start a Pilates-based rehab program to prevent a reoccurrence of your symptoms then come and see one of our highly qualified physios today [ Click here to Request an Appointment ]
Facet Joint Pain
Our facet joints are the lesser known little brother to the spines intervertebral joints: formed by a disc and two adjacent vertebrae. If we were to look down the spine, the intervertebral joints sit in “front” of the spinal cord and the facet joints sit at the “back”. Our facet joints change in orientation as we move up the spine and it is this orientation change that dictates the type of movement that occurs in different segments of the spine: be it flexion, extension, side-bending or rotation. The role of the facet joints, of which there are two, a right and a left, at each spinal level is to guide and limit movement at that level.
Over time or in response to an acute injury our facet joints can become sources of pain. Injured facet joints are typically either hypomobile – stiff; or hypermobile – loose.
Risk Factors / Causes:
Acute injury such as a sprain to the joint can occur due to a twisting or high loading movement that overloads the tissues of the facet. Each facet joint has a low-friction cartilage and is surrounding by a capsule which lubricates the joint. The capsule is richly innervated by tiny nerves which provide a warning when irritated.
Unstable or degenerated intervertebral joints can place extra strain on the facet joints resulting in an acute overload injury.
Management:
An irritated or inflamed facet joint often drives a powerful spasm response in the muscles parallel to the spine causing pain, movement loss and “crooking” of normal posture. Our first response as physiotherapists is to relax the muscle spasm, restore mobility to stiffened segments and provide pain relief.
Our assessment will have told us whether stiffness or hypermobility, or a combination of the two, are an issue so we mobilise the stiff and utilise stabilising exercises to support the loose. In doing so we provide pain-management; we restore optimal joint movement; normalise muscle recruitment patterns; and enhance core stability. All of these techniques are gradually progressed until we are replicating the loads that would be experienced in a work, leisure or sport environment. Many of our patients with facet joint pain respond well to Pilates-based exercise to improve their muscle strength and endurance and general joint and body mobility.
Where facet joint injury occurs secondary to injury to or degeneration of the intervertebral joint we address this as an equal priority to lessen the chance of reoccurrence.
If you’re suffering from facet joint pain or would like to start a Pilates-based rehab program to prevent a reoccurrence of your symptoms then come and see one of our highly qualified physios today [ Click here to Request an Appointment ]
Chronic
Spondylolysis
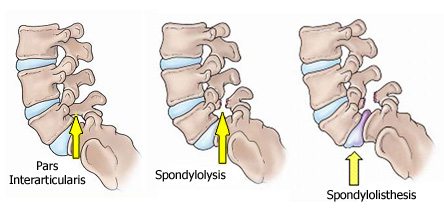
A spondylolysis, also known as a pars fracture, is a stress fracture occurring in a spinal vertebra. Whilst this type of injury only effects 3-6% of the population its incidence in young athletes can be up to 15%. The vast majority of spondylolytic defects occur at the L5 vertebra of the lower back, and are usually discovered during investigation into a complaint of lower back pain.
Apart from pain, although some people remain asymptomatic, our main concern with a spondylolysis is that it can lead to a spondylolisthesis (insert hyperlink) or forward slipping of one vertebra relative to the one adjacent.
Risk Factors / Causes:
Some people are born with a pars defect; at the other end of the timeline we have pars fractures occurring due to age-related degenerative spinal changes; occasionally it’s in response to trauma; and the most common cause is overuse injuries in athletes such as cricketers, divers or gymnasts.
A spondylolysis is an overuse injury where training load exceeds the body’s capacity to adapt. Repeated loading of the pars interarticularis of the vertebral arch leads to extensive microtrauma in turn causing pain, inflammation and bone disruption. It’s worth noting that stress and microtrauma are the stimuli by which fitness improves, bones become stronger and muscles grow and adapt. However, this mechanism is reliant upon rest and recovery – when the load, whether acutely or cumulatively, exceeds the ability to recover injury ensues.
Poor technique – particularly for fast-bowlers in cricket or over-rotation in gymnasts or divers; lumbar muscle tightness and or weakness; poor core strength; and increasing training volume too quickly are all contributing factors in the development of a spondylolysis.
Management:
Patients presenting to Construct Health with a spondylolysis often are in a lot of pain, so we use techniques to reduce muscle spasm, support posture and reinforce pain-relieving movement patterns. Lumbar extension is often acutely painful so we are mindful of avoiding extension during the early stages of rehabilitation.
In addition to pain-management we look to restoring optimal joint movement; normalising muscle recruitment patterns; and enhancing core stability. All of these techniques are gradually progressed until we are replicating the loads that would be experienced in a work, leisure or sport environment. Many of our patients with spondylolysis respond well to Pilates-based exercise to improve their muscle strength and endurance and general joint and body mobility.
As this injury is often technique-driven or relates to poor training structure we work closely with coaches to manage the athlete and allow training to continue during the acute phases; identify and correct technique faults; and to appropriately challenge the athlete as recovery progresses.
If you’re suffering from spondylolysis or would like to start a Pilates-based rehab program to prevent a reoccurrence then come and see one of our highly qualified physios today [ Click here to Request an Appointment ]
Spondylolisthesis
In describing a spondylolisthesis we refer to it as being a “slip” of one vertebra relative to its neighbour. Many people with a spondylolisthesis can be symptom free for years, with the condition becoming painful only as the degree of slippage increases thus placing stress on surrounding tissues.
Risk Factors / Causes:
This slip occurs following a fracture (spondylolysis – insert hyperlink) or as a result of a congenital defect in the pars interarticularis of the vertebral arch and is most commonly found in the fifth lumbar vertebra where it articulates with the sacrum or tailbone.
Because a spondylolisthesis develops from a spondylolysis they share the same risk factors and causative mechanisms. To recap: some people are born with a pars defect; at the other end of the timeline we have pars fractures occurring due to age-related degenerative spinal changes; occasionally it’s in response to trauma; and the most common cause is overuse injuries in athletes whose sport involves high-speed high-load hyperextension and rotation of the spine such as cricket fast bowlers, divers and gymnasts.
A spondylolysis is an overuse injury where training load exceeds the body’s capacity to adapt. Repeated loading of the pars interarticularis of the vertebral arch leads to extensive microtrauma in turn causing pain, inflammation and bone disruption. It’s worth noting that stress and microtrauma are the stimuli by which fitness improves, bones become stronger and muscles grow and adapt. However, this mechanism is reliant upon rest and recovery – when the load, whether acutely or cumulatively, exceeds the ability to recover injury ensues.
Poor technique – particularly for fast-bowlers in cricket or over-rotation in gymnasts or divers; lumbar muscle tightness and or weakness; poor core strength; and increasing training volume too quickly are all contributing factors in the development of a spondylolysis and in turn a spondylolisthesis.
Management:
Patients presenting to Construct Health with a spondylolisthesis often are in a lot of pain, so we use techniques to reduce muscle spasm, support posture and reinforce pain-relieving movement patterns. Lumbar extension is often acutely painful so we are mindful of avoiding extension during the early stages of rehabilitation.
In addition to pain-management we look to restoring optimal joint movement; normalising muscle recruitment patterns; and enhancing core stability. As the deep core muscles are the primary mechanism responsible for controlling slippage we spend a lot of time focusing on muscle retraining as part of our patients’ rehab. All of these techniques are gradually progressed until we are replicating the loads that would be experienced in a work, leisure or sport environment. Many of our patients with a spondylolisthesis respond well to Pilates-based exercise to improve their muscle strength and endurance and general joint and body mobility.
As this injury is often technique-driven or relates to poor training structure we work closely with coaches to manage the athlete and allow training to continue during the acute phases; identify and correct technique faults; and to appropriately challenge the athlete as recovery progresses.
In a small number of cases surgery is required to address the underlying cause of the patients’ symptoms. This is quite rare in the young spondylolisthesis patient but is one of the main reasons for spinal procedures in the elderly. The surgery may be a stabilisation procedure; a fusion; or a decompression procedure such as a laminectomy. Once the surgery has been performed we begin a process of rehabilitation that is very similar to what we undertake for the non-surgical patient: that is focusing on pain-management; re-education of movement patterns; improved core control; muscle strengthening and endurance training; and a return to full normal function
If you’re suffering from spondylolisthesis or would like to start a Pilates-based rehab program to prevent a reoccurrence then come and see one of our highly qualified physios today [ Click here to Request an Appointment ]