A dislocated elbow is not a pretty sight. My most vivid memory of an elbow dislocation was of a pole-vaulter asking me to “pop” his freshly dislocated elbow back in. He had stalled at the top of the vault and had fallen onto the track below. Rather than doing as he asked, I checked his pulse, sat him down with an ice pack and called a mate who is an orthopaedic surgeon and arranged for an emergency consult. Elbow dislocations can be problematic as they often result in bony fractures; damage to the joint surfaces and the peripheral nerves and blood vessels.
Risk factors / Causes:
One could argue that taking up pole vaulting is a risk factor but apart from that we are dealing with a fairly uncommon injury. Previous elbow dislocation or general joint or tissue hypermobility may predispose an individual to dislocation.
The mechanism of injury is usually a fall onto an outstretched hand (our old friend FOOSH) plus or minus rotation.
Passengers in motor vehicle accidents can present with elbow dislocations due to reaching out towards the dash or seat in front to lessen the impact.
Management:
For a simple dislocation without bony or ligamentous injury the joint may be “popped” back in place – this is done under sedation and with sufficient pain medication on board. Once the joint is stable, the rehabilitation process begins to manage pain and restore range, strength and power.
Where surgery is required the process is much longer and depends on the extent of nerve, or other damage. Once rehab begins the same rules apply in that we aim to manage pain and restore range, strength and power. Unfortunately full restoration of range is not always possible following dislocation. The good news is that for most people a mild loss of extension or rotation at the elbow doesn’t hinder their usual sporting or daily activities.
N.B – It’s worth noting that we have been discussing elbow dislocations in adults. Kids are another matter entirely. Elbow dislocations are the most common dislocation in children. They usually occur when the parent attempts to lift a child by the hand and the loose connective tissue allows the joint to dislocate. These injuries are simple to relocate and the child will, as a rule, suffer no ill effects.
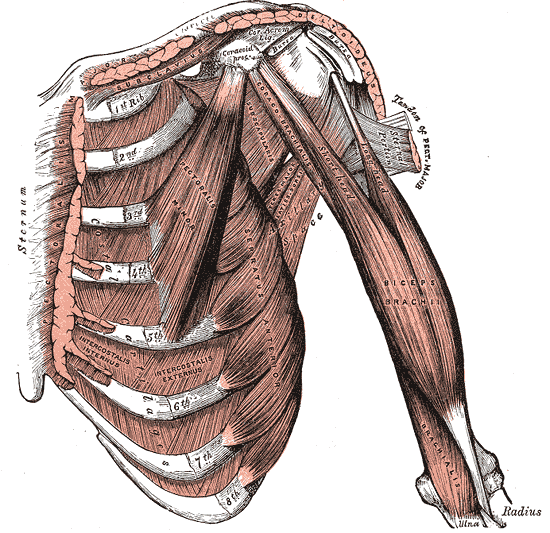
As a rule a complete bicep tendon rupture at the elbow is a fairly easy diagnosis. You ask the patient to flex the bicep against resistance and up pops a golf-ball shaped Popeye of a muscle rather than the elongated muscle belly that we usually see. Partial tears are a little trickier and may require scanning to give a definitive diagnosis, but the patient’s story of how they hurt themselves – the elbow forced straight against resistance; their age – middle-aged and older; their gender – male; signs and symptoms – weakness, tenderness and bruising over the insertion point of the muscle – all point towards a tear.
Risk Factors / Causes:
We usually see bicep tears in middle-aged and older males after they’ve lifted an object heavier than expected – suitcases are a good one; or associated with a fall where they have attempted to arrest the fall by grabbing onto a railing and in the process overloaded the bicep tendon leading to rupture. Smoking and corticosteroid use are associated with an increased risk of tendon damage.
The younger blokes who show up with a torn bicep usually do so courtesy of a rugby union or rugby league tackle gone wrong. This usually involves throwing the arm out in a last gasp attempt to tackle an attacker who has stepped around them.
Management:
For the younger guys this is usually managed with a surgical repair. The tendon is reattached to the bone and the arm is then immobilised for up to six weeks. Rehabilitation focuses upon a very gradual reintroduction of load with a concomitant focus upon regaining range of movement at the elbow
Many patients with a torn distal bicep elect to manage the rehabilitation process non-surgically. With conservative management (non-surgical) we see a 30-40% loss of strength but pretty good range of motion. With these patients we work on strengthening the nearby muscles in order to compensate for the loss of bicep strength. We also work to improve scapular control (shoulder – shoulder-blade); posture and the mobility of the thoracic and cervical spines as these structures take on a greater compensatory role.
If you’ve ruptured your bicep or are in post-op recovery then come and see one of our highly qualified physios today [ Click here to Request an Appointment ]
Chronic
Tennis Elbow
People are often quietly relieved to be told they have tennis elbow. Everybody’s heard of it, though few know what it is, they’re relieved that it’s not something worse – though of course, for some people it can be the source of significant pain and discomfort. We’ve listed this in the chronic section although it can be and of course starts out as an acute injury. It is however one of those injuries that people will often underestimate, ignore and by the time they present to us it has become chronic.
Risk Factors / Causes:
Tennis elbow on one level is an irritation of the muscles, tendons, tendon sheath and attachment point (the epicondyle) for the wrist and finger extensors. On another level many of the symptoms of tennis elbow are due to restrictions in nerve tissue as it passes around the elbow. People with tennis elbow that has a significant nerve restriction component are often surprised when we start treating their neck to fix their elbow – it’s “I know this looks funny but trust me” time.
Why do people get it? The forearm component occurs when someone performs a task that involves lots gripping or repetitive movements of the wrist and hand such as a DIY house painter. Tennis, obviously, particularly with a non-regular/non-player unaccustomed to the sport and with poor technique.
A stiff, restricted cervical spine contributes to a loss of normal function and movement of the peripheral nerves leading to a “neural” tennis elbow.
Management:
We start with a thorough assessment to work out how much of this is from the neck and how much from the elbow. Once we know this we can formulate a plan to control pain and improve function. With nerve restriction we directly treat the neck as well as any muscle or joint junctions that may impact upon the pathway of the nerve as it exits the neck and makes its way down through the shoulder and arm. Patients are shown nerve mobilisation techniques that they use as part of their at-home rehab program.
Where the forearm is largely at fault we use techniques to release the soft tissue and mobilise restricted joints at the elbow and wrist. Most importantly we look at the technique that contributed to the fault in the first place. Improving poor technique will help a condition to heal more quickly and it will help prevent its reoccurrence.
As the patient improves we reintroduce strength and endurance work and transition them back to full work or play.
If you think you’re suffering from a case of tennis elbow then come and see one of our highly qualified physios today [ Click here to Request an Appointment ]
Golfer’s Elbow
Golfer’s Elbow is the lesser known sibling of tennis elbow. Tennis elbow effects the outside and golfer’s elbow the inside of the elbow at the bony bump known as the medial epicondyle.
Risk Factors / Causes:
Golfer’s elbow on one level is an irritation of the muscles, tendons, tendon sheath and attachment point (the epicondyle) for the wrist and finger flexors. On another level many of the symptoms of golfer’s elbow are due to restrictions in nerve tissue as it passes around the elbow. People with golfer’s elbow that has a significant nerve restriction component are often surprised when we start treating their neck to fix their elbow – it’s “I know this looks funny but trust me” time.
Why do people get it? The forearm component occurs when someone performs a task that involves lots gripping or repetitive movements of the wrist and hand such as a DIY house painter. Golf, obviously, particularly with a non-regular/non-player unaccustomed to the sport and with poor technique.
A stiff, restricted cervical spine contributes to a loss of normal function and movement of the peripheral nerves leading to a “neural” golfer’s elbow.
Management:
We start with a thorough assessment to work out how much of this is from the neck and how much from the elbow. Once we know this we can formulate a plan to control pain and improve function. With nerve restriction we directly treat the neck as well as any muscle or joint junctions that may impact upon the pathway of the nerve as it exits the neck and makes its way down through the shoulder and arm. Patients are shown nerve mobilisation techniques that they use as part of their at-home rehab program.
Where the forearm is largely at fault we use techniques to release the soft tissue and mobilise restricted joints at the elbow and wrist. Most importantly we look at the technique that contributed to the fault in the first place. Improving poor technique will help a condition to heal more quickly and it will help prevent its reoccurrence.
As the patient improves we reintroduce strength and endurance work and transition them back to full work or play.
If you think you’re suffering from a case of golfer’s elbow then come and see one of our highly qualified physios today [ Click here to Request an Appointment ]


























{kind=link}