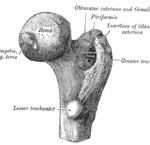
A hip fracture is a break in the upper quarter of the thigh bone. These breaks typically happen in the elderly although may be seen as the result of trauma or stress in younger populations.
Risk Factors / Causes:
Our patients will tell us that they fell over and fractured their hip and whilst this is true, the opposite is often equally the case – osteoporotic weakening of the bone will cause a fracture as the person places load through the leg causing them to fall over. Osteoporosis results from either a low peak bone mass or loss of bone mineral mass with ageing. Risk factors for osteoporosis include being female, particularly post-menopause; a history of alcoholism or anorexia; being Caucasian or Asian; hyperthyroidism; smoking; limited weight-bearing exercise; and the use of steroids and other medication.
Younger endurance athletes may present with a hip fracture, particularly where there is a history of anorexia, amenorrhea and overtraining. The hip fracture is the end result of an ongoing stress injury due to overloading; insufficient recovery; and an inadequate diet.
Fractures are seen in bones weakened by tumour metastasis.
Management:
In most cases a hip fracture is stabilised surgically, the exception exists where the patient is too ill to undergo surgery or is wheelchair or bed-bound and has a relatively stable fracture without significant pain.
Physio begins on the day of the operation. At first the physios’ role is to assist the patient to overcome the effects of the surgery. We get the patient up and moving to help promote healing and prevent infection and other secondary disorders that can occur as a consequence of trauma, anaesthesia and immobilisation. Over time we work with the patient to regain movement of the hip and leg to promote pain management and fluid clearance. As healing continues our focus is to regain movement and strength of the hip, knee and ankle joints. The actual timeline of recovery depends upon the exact location of the fracture; the surgical method used to achieve stabilisation of the hip; and the health of the patient.
When hip fractures occur as a result of overtraining for sport, we need to put a lot of energy into designing a rehab program that maximises the return to full function but doesn’t reinforce the behaviour pattern that lead to the hip fracture in the first place. This includes the involvement of sports psychologists, doctor, dietitians and other health professionals to best manage the rehabilitation process.
In the majority of cases the patient will regain much if not all of the strength and mobility that they had prior to fracturing the hip.
If you’ve fractured your hip and need help with your post-surgical rehab then come and see one of our highly qualified physios today [ Click here to Request an Appointment ]
Adductor (groin) Strain
The subject of a thousand lame jokes, the strained groin, as you’d know if you’ve ever experienced one, is in fact no laughing matter. A recent or poorly rehabilitated hip adductor (groin) strain can significantly limit the ability to run, kick or change direction with any confidence.
Risk Factors / Cause:
Groins strains are really common in sports that require rapid acceleration, change of direction and kicking. We see them in all of the major ball sports and like their close cousin the hamstring strain contributing factors include: fatigue; inadequate warm-up; poor core stability; pre-existing injury and a history of lumbar spine dysfunction or injury.
Management:
The first step is to control the extent of injury through rest/ice/compression and elevation (RICE) and the often neglected, avoidance of alcohol and other aggravating factors.
Physiotherapy treatment will focus upon restoration of muscle length, muscle strength, endurance and coordination. This occurs in conjunction with assessment and treatment/management of lumbar spine pathology and the associated restrictions in mobility and function of the nerve tissue as it exits the back and makes its way through the leg.
As the patient progresses treatment begins to address sports-specific factors such as running technique and lower limb biomechanics. In many cases ongoing management through Pilates, stretching, strengthening and hands-on physio keeps the athlete on track
Think you’ve strained your groin or need help to stop it happening again then come and see one of our highly qualified physios today [ Click here to Request an Appointment ]
Chronic
Osteitis Pubis (OP)
The scourge of the ageing professional AFL player – osteitis pubis is an inflammatory condition effecting the point at which the bones of the pelvis come together.
Risk Factors / Causes:
Osteitis pubis is an overuse condition where repeated stress without sufficient recovery leads to inflammation, irritation and in severe cases bone degradation at the pubic symphysis.
It frequently occurs in AFL, and other football players, who have a history of groin strains, hernia or lumbo-pelvic injury or instability. The reason for its prevalence in AFL players is the high-degree of unilateral loading of the pelvis (i.e. they do a lot of kicking with one leg). It should be noted that the incidence of osteitis pubis in professional AFL players has fallen over the last five years due to better screening of at-risk individuals and the development of injury prevention plans aimed at preventing its onset.
Management:
Rest, rest, rest is step one; closely followed by step two: assess, assess, assess. The tissue needs rest to allow the inflammation to settle and pain to be better managed; we need to assess through specific physiotherapy tests and medical imaging such as x-rays, MRI or CT scans to determine the best management strategies to adopt.
Some patients will have anti-inflammatory medications injected into the tissue surrounding the pubic symphysis and in severe or non-responsive cases surgery may be required.
As with all of our patients, we aim to return the individual to their pre-injury level of work or sporting function. With OP this requires lots of specific work to deload the stressed tissues; restore length and strength to the muscles of the groin, hip and pelvis; improve core control; and address any underlying lower limb biomechanic issues contributing to asymmetric loading of the pelvis. We do this through a combination of Pilates and home or gym-based exercise to improve muscular strength, endurance and power.
As our patient with osteitis pubis recovers we gradually reintroduce sports-specific training, all the while monitoring for any change in symptoms or movement form or function. If there is any increase in pain or a noticeable change in muscle tightness or loss of running technique we drop the training load, increase treatment and adjust our plans accordingly.
Think you need help to get on top of a case of osteitis pubis then come and see one of our highly qualified physios today [ Click here to Request an Appointment ]
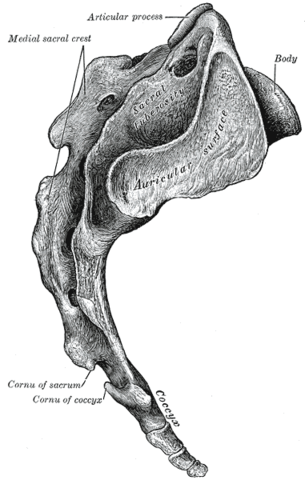
Sacroiliac Joint (SIJ) Pain
We’ve listed this as a condition relating to the hip where as in many ways it can be equally thought of as a type of back pain. The sacroiliac joint or SIJ, of which we have two, is the joint formed by the union of the sacrum (tailbone) and the ilium (hip or pelvic bone). It’s a highly stable joint that allows only a minor degree of movement but its importance lies in its near constant motion as we walk, run, climb stairs, move from sitting to standing, jump, hop and so on. As we perform all of these tasks the sacrum, which if you’ll recall lies wedged between the two hip bones, rocks forward and back and moves through a number of rotational planes. Dysfunction in this complicated pattern of movement is believed to be the source of considerable lower back and buttock pain. The typical SIJ dysfunction is one of hypermobility that leads to an unstable lumbo-pelvic platform. An unstable pelvis is one that is less able to safely absorb the loading patterns that occur through the body as we move.
Risk Factors / Causes:
SIJ dysfunction and SIJ pain can arise from: arthritic changes in the joint; spinal surgery; leg length discrepancies; repetitive loading (e.g. running – particularly with poor technique); scoliosis; pregnancy – due to weight gain, postural changes and hormone-induced laxity of ligamentous and connective tissue during the final trimester; trauma; and poor core muscle strength and endurance.
Management:
As in everything we treat the first steps involve managing the pain and associated disability but the real trick is to dig down to the root cause of the problem.
If it’s poor biomechanics when running; poor core strength or altered muscle recruitment patterns; muscle imbalances; obesity; inadequate task rotation at work; having one leg longer than the other OR as is often the case a combination of all of the above, we work with the injured person to address all of these factors to return them to full healthy pain-free functioning.
The treatment process itself will generally involve deloading the aggravated tissues; mobilisation of stiff joints; correction of leg length discrepancies; providing external stability through taping or the use of an SIJ stabilising belt; and providing internal stabilisation through training of the deep core muscles including the multifidus and the transverse abdominis.
Patients who don’t respond to conservative treatment may benefit from a number of approaches designed to interfere with either the inflammatory process or with the pain-signalling system. This can include nerve blocks, steroid injections, or denervation procedures which destroy the nerve branch innervating the SIJ. Once these procedures are complete we continue with conservative management.
As the symptoms improve we work with the patient to gradually reintroduce them to sport, work and the normal activities of daily living. Over time the patient is able to return to their pre-injury status and in some cases are fitter, stronger and healthier than before
Think you have SIJ pain or dysfunction and/or need help with your post-injury rehab come and see one of our highly qualified physios today [ Click here to Request an Appointment ]