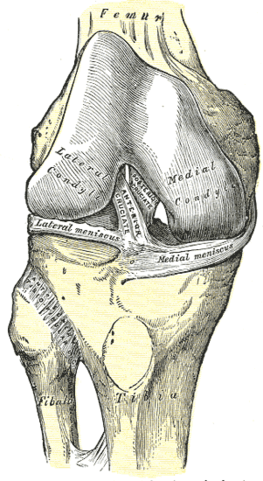
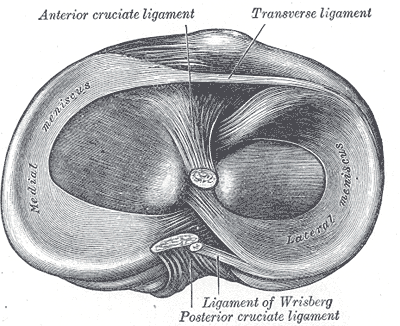
If you have a few spare moments scroll through the Rugby League Week “Casualty Ward” page and sandwiched in-between the shattered limbs and dislocations you will find no fewer than 13 season ending ACL injuries. So what is the ACL and why is damage to this structure the cause of so much grief for the professional or amateur athlete. The ACL is one of the main ligamentous stabilisers of the knee – it prevents excessive movement of the joint particularly as it relates to pivoting or rotational movement. Without a functioning ACL the footballer, netballer or tennis player is generally unable to change directions or pivot at speed and hence are incapable of competing at a high level.
Risk Factors / Causes
In the majority of cases an athlete experiences a ‘non-contact’ rupture of the ACL where the ACL ruptures because it is unable to cope with the shearing and rotational forces generated during a high speed change of direction not because of an external force applied during a tackle. Athletes with a previous history of ACL rupture, even of the opposite leg, are at a higher risk of ACL injury, as are females competing in competitive sport.
Management
This is where it gets interesting. If your work or sport requires a reliably stable knee or you are experiencing episodes of knee instability in everyday life then a surgical reconstruction is the best management strategy. For many people, adopting a conservative (non-surgical) approach involving extensive rehabilitation of the injured knee will suffice. Anecdotally we have seen some evidence of increased osteoarthritic (OA) complications in the conservatively managed knee however this may be attributable to injuries sustained to the cartilage and bony tissue at the time of ACL rupture and not the rupture and associated instability itself. Plenty of people opt for a surgical ‘wash out’ of the knee without undergoing the full ACL repair and this does seem to address the OA concerns.
In either a surgical or conservative case the aims of physiotherapy are much the same: manage pain; restore range of movement; develop power, agility, balance and endurance.
Think you’ve ruptured your ACL or are post-ACL reconstruction and need some help with your rehab then come and see one of our highly qualified physios today [ Click here to Request an Appointment ]
Meniscal Tear
Scourge of football players and the weekend warrior-class, the meniscal tear is a tear of the shock absorbing discs that sit between the thigh and shin bones.
Risk Factors / Causes
Like most knee injuries a meniscal tear occurs when a rotational or twisting force is applied to a flexed knee. This can occur in a non-contact scenario – sudden change of direction; or a contact scenario – a tackle.
Management
Minor meniscal tears can be managed through physiotherapy-led rehab to strengthen and mobilise the knee. Where a significant tear has occurred, particularly if this causes ongoing pain or episodes of instability or ‘locking’ of the knee, then surgery is required.
In either a surgical or conservative case the aims of physiotherapy are much the same: manage pain; restore range of movement; develop power, agility, balance and endurance.
Think you’ve damaged your meniscus or need post-op rehab then come and see one of our highly qualified physios today [ Click here to Request an Appointment ]
Chronic
Arthritis
Osteoarthritis (OA) is a condition resulting in joint pain and stiffness and plays a significant role in loss of mobility and independence in the elderly. OA of the knee is a degenerative condition effecting the joint surfaces of the femur, the tibia and the patella.
Risk Factors / Causes:
As we age, we get the double-whammy of a reduction in the ability for our body to repair itself occurring alongside an accumulation of wear-and-tear. These factors are heightened when a person is obese or overweight and if there has been a history of damage to the joint surfaces.
As these degenerative changes accumulate, the normal pattern of movement is altered in response to which the body lays down bone (spurs) which in turn become a source of irritation and inflammation. Nasty little cycle.
Management:
As physios we aim to keep people moving well throughout the lifespan. With OA of the knee our focus is to restore function and reduce pain. We do this by lengthening and strengthening muscles; improving balance and proprioception; teaching self-massage and self-stretching techniques; and educating people regarding the importance of healthy eating and exercise to maintain an ideal weight.
With advanced OA, surgery to remove inflamed and damaged tissue or to “replace” the joint may be required. There are a number of different surgical methods used to manage OA but the aim of all is to improve joint function and to reduce pain. Post-surgical rehabilitation is imperative but often overlooked or underappreciated. Its importance is due to the widespread biomechanic changes that are present with advanced OA. People have muscle loss and wasting; poor balance and proprioception; poor joint mobility and alignment – all of these need to be addressed in addition to having surgery.
If you’re experiencing the symptoms of knee OA or need post-op rehab then come and see one of our highly qualified physios today [ Click here to Request an Appointment ]
I get worried when a patient tells me that they have a “syndrome”. A “syndrome” diagnosis can be the means by which a lazy or poorly informed practitioner throws into one basket all of the conditions relating to that particular joint, tissue-type, organ or structure. PFS is a great example of this, as it is a catch all phrase for pain felt behind the kneecap (the ‘retropatellar’ surface). Over the years we’ve seen patients present with a PFS diagnosis who have advanced osteoarthritis, others with acute damage to the retropatellar surface following a knee dislocation and my personal favourite – the ACL deficient knee diagnosed as PFS. Now, whilst many of the signs associated with PFS were present in each of the above examples, the management of the underlying cause differed greatly in each case. At Construct Health we’re big fans of treating the cause rather than the symptoms.
The typical PFS symptoms are pain around or behind the kneecap following or during weight-bearing such as walking, running, hopping and climbing or descending stairs. They can also be present at rest or with sustained postures such as sitting for a long time with the knee bent – think long haul flight or sitting in a cinema seat.
People with PFS will often be told that they have an alignment or tracking problem with the knee. This is largely true, in that muscle and connective tissue imbalances or restrictions cause the patella to track imperfectly as the knee bends and straightens.
Management
The cardinal rule at Construct Health is that the “why” is just as important as the “what”. We treat what is wrong – pain, imbalance and inflammation – and we find out why it’s gone wrong and work to fix that too. Where we can’t fix the underlying problem, for example in cases requiring surgical repair of damaged or degraded tissue, we refer on and assist with the post-surgical rehab.
We work with the patient to improve control, strength and endurance of the muscles around the pelvis, leg and core. A particular focus is on the medial or inside knee muscles, glutes and calves. We stretch and release the tight, weak muscles on the outside of the legs; we improve the range of motion in the joints of the foot and ankle and use taping or orthotics for the arch of the foot to correct poor biomechanics
Iliotibial (ITB) Syndrome (there’s that syndrome word again) is an overuse injury effecting the outside of the knee. The ITB is a band of connective tissue running down the outside of the leg from the hip to the knee that, when tight, can cause friction as it slides over the bony outside of the knee. It is the friction that causes irritation, inflammation and pain.
Risk factors / Causes:
ITB Syndrome is a biomechanical disorder that occurs due to a number of factors including: imbalances in the core, hip, pelvis and leg muscles; poor foot control; poor running technique; excessive mileage; worn-out shoes and fatigue.
Management:
This is a tricky one – ITB Syndrome management is both very simple and at times complex. Some people have beautiful running technique when fresh, but terrible technique at speed, up or down hills or when fatigued; others have fine technique but weakness and/or tightness in a particular muscle group; others simply need a new pair of shoes. Whatever the case may be its imperative to get to the cause of the problem and do more than treat the symptoms.
However, we do of course manage the symptoms and this generally involves deloading the tight structures of the outside of the hip and thigh thus limiting friction at the knee.
Once the symptoms and what are believed to be the underlying causes are managed it’s important to push the runner into situations which challenge their biomechanics – so we assess running technique under fatigue, speed and high-loading (e.g. downhill running) and see if things hold up. If not, we back off the loading, treat and give more strengthening, lengthening and endurance training until the runner is able to maintain technique under all circumstances.
Osgood Schlatter’s Disease in an inflammatory condition affecting the growth plate on the tibia or shin bone at the point at which the patella tendon inserts. OSD is part of a family of growth plate disorders that occur during adolescence particularly in active kids hitting their peak growth phase.
Risk Factors/Causes
Kids who play lots of running and jumping sports and who have poor lower limb biomechanics are at greatest risk of developing OSD. The growth plate in question is at the front of the shin bone at the insertion point of the patella tendon. Prolonged or frequent loading through the tendon, as occurs with running and jumping, can overload the tissues of the growth plate resulting in an inflammatory response.
Management
OSD is a self-limiting condition that is fully resolved by the time the growth plate fuses but in the mean-time the condition must be managed to allow the individual to continue to play sport, exercise and enjoy a pain-free adolescence.
The first, and perhaps hardest step for the active adolescent is to reduce the amount of sport or exercise they are participating in. What we usually do is ask the individual to list all the sport/exercise they play and rank them from least to most important/enjoyable – the ones at the bottom of the least get scratched and as necessary you continue up the list, hopefully stopping before the top.
We then work to address factors contributing to the condition including poor foot and lower limb biomechanics; restricted neural tissue; poor balance and proprioception; restricted joint range of motion or muscle length and cardiovascular fitness.
As pain resolves and strength and power return to the affected limb(s) we gradually reintroduce the activity that was taken out at the beginning of the rehab phase whilst keeping a close eye on any aggravation of symptoms.























{kind=link}