The high ankle or syndesmosis sprain is an injury to the ligaments that bind the two bones of the lower leg – the tibia and fibula – together at their lower end. We see plenty of these in footballers as the result of a collision or tackle.
Risk Factors / Causes:
A syndesmosis sprain occurs when a twisting force is applied to the outside of the leg whilst the foot is planted on the ground. They are also seen when the foot is forcibly pushed upwards, literally forcing the bones apart – aside from the typical footy injuries, these are quite common in mountain bikers courtesy of poorly executed landings from jumps.
Management:
In severe cases, where the ankle has become grossly unstable, a surgical repair is undertaken to screw the tibia and fibula back together. The screw is usually removed 12 or so months after the initial operation, by which stage there should be sufficient healing to safely stabilise the joint.
Good management starts immediately at the time of injury with the ever reliable rest (R), ice (I), compression (C), and elevation (E). Get this part right and your recovery time can be dramatically reduced. With a high ankle sprain the patient is usually provided with a “moon” boot or crutches to limit loading of the painfully injured limb.
Physiotherapy treatment to reduce inflammation and manage pain starts early on and as recovery progresses the physiotherapist works with the patient to restore muscle length, restore tendon and muscle strength and regain joint range of motion.
We then work to address factors contributing to the original injury including poor foot and lower limb biomechanics; restricted neural tissue; balance and proprioception; and cardiovascular fitness.
The last, and often overlooked, component of rehab is sport, work or lifestyle-specific retraining. If your job has you walking on uneven ground; you live in a high-set house and run up and down stairs all day long; or you play in the NRL and need to regain full explosive agility – whichever it might be we work with you to return you to your full pre-injury level of function.
Think you’ve sustained a high-ankle (syndesmosis) sprain or need help with your post-injury rehab come and see one of our highly qualified physios today [ Click here to Request an Appointment ]
Chronic
Shin Splints
Shin splints is an easy one to explain as pretty much everyone has either had them or knows someone who has. In the Construct Health clinics we typically see shin splints at the start of the summer or winter sporting seasons as training loads increase and in some people this is the first warning sign of too much too soon.
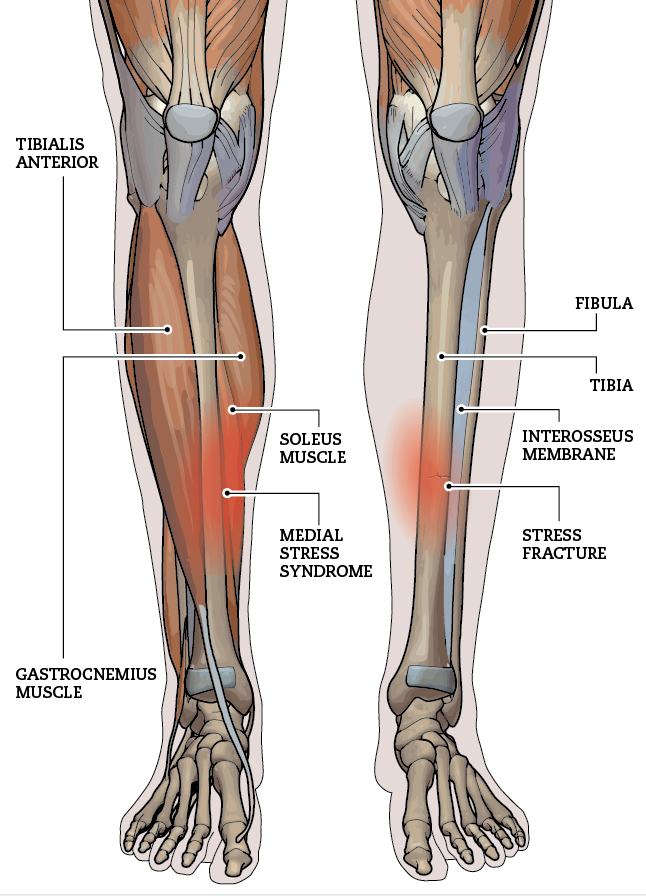
The pain presents as a dull ache in the shin following running or other loadbearing exercise. At first, the symptoms disappear following a good warm-up but over time if not treated it can become a constant pain, occasionally symptomatic of a stress fracture.
Risk Factors / Causes
Shin splints are an overuse injury where training load exceeds the body’s’ capacity to adapt. The tibialis anterior, the tibialis posterior and the connective tissue surrounding the shin (the anchor point for these muscles) become overworked, suffering extensive microtrauma leading to pain and inflammation. It’s worth noting that stress and microtrauma are the stimuli by which fitness improves and muscles grow and adapt. However, this mechanism is reliant upon rest and recovery – when the load, whether acutely or cumulatively, exceeds the ability to recover injury ensues.
Poor lower limb and foot biomechanics; inappropriate footwear; running on hard or sloping surfaces; leg and core muscle tightness and or weakness; increasing training volume too quickly are all contributing factors in the development of shin splints.
Management
Ice, ice baby. Yes Vanilla said it all – ice them shins up good and proper. Be it ice baths, ice packs or ice massage these bad boys respond well to icing. As always be careful of ice burns, so don’t apply directly to the skin; check skin regularly; don’t ice for prolonged periods and be particularly careful if you are sensitive to ice or have decreased sensation due to an underlying condition such as diabetes.
Even if the shin pain prevents you from running there’s lots to do in terms of addressing the underlying causes such as Pilates to improve core muscle control; stretching and strengthening of tight, weak muscles in the legs; improving the range of motion in the joints of the foot and ankle and taping or orthotics for the arch of the foot to correct poor biomechanics
Often if the shin splints aren’t severe, management is treat and train; the more severe the case the less exercise the patient can do. Either way we gradually increase training loading in a way that places stress on the system without overwhelming it and causing a reaggravation.
Think you’ve got shin splints or are about to start training and need help preventing their return then come and see one of our highly qualified physios today [ Click here to Request an Appointment ]
Stress Fracture
The lower limb stress fracture is the far end of the spectrum described in the shin splints section. It shares the same causes, many of the same risk factors and much of the same treatment. They most commonly occur in the tibia bone of the shin; and the navicular and metatarsal bones of the foot.
Where they differ is the increased incidence amongst female athletes attributable to hormone and behaviourally-related decrements in bone mineral mass. Female athletes when compared with men and their non-athletic female counterparts are reportedly more likely to present with eating disorders, irregular menstrual cycles (amenorrhea) and reduced bone density or osteoporosis.
As already stated much of the management is very similar to that for shin splints or any overtraining injury. However in some cases the following professionals need to be consulted to ensure the proper course is charted: a GP or sports physician; general or sports psychologist; dietitian; surgeon and podiatrist.