The bones of the spine are very strong but like any other of the body’s bones are susceptible to fracture. Crush or compression fractures are commonly seen in the lower of the thoracic vertebra and can cause strong localised pain and pain, numbness and weakness away from the injury site if the spinal nerves at the level of injury are compromised.
Risk Factors / Causes:
Thoracic crush fractures often occur when a downward pressure is applied to a bent spine. An example is falling off of a chair onto the floor – when this occurs the head typically comes forward as the buttocks hits the floor.
Fractures can also occur with any fall from a height and from a car accident or similar trauma.
Osteoporosis is the greatest risk factor for thoracic fractures. The weakened bone is unable to absorb the forces applied to it and fails, leading in some cases to a rounded hunched posture known as a thoracic kyphosis or “Dowagers Hump”.
It is worth noting that female athletes are at a greater risk of thoracic fractures due to potential decrements in bone mineral density. Female athletes when compared with men and their non-athletic female counterparts are reportedly more likely to present with eating disorders, irregular menstrual cycles (amenorrhea) and reduced bone density or osteoporosis.
Management:
As in everything we treat the first steps involve managing the pain and associated disability.
The treatment process itself will generally involve deloading the aggravated tissues and providing internal stabilisation through training of the deep spinal extensor muscles.
In the elderly, weight-bearing exercises are integral in preventing the worsening of osteoporosis. Walking, weight-training, Pilates and Tai Chi are all excellent components of a structured rehab program.
Our elderly patients are often significantly deconditioned so as their symptoms improve we work to gradually reintroduce them to sport, work and the normal activities of daily living. Over time the patient is able to return to their pre-injury status and in some cases are fitter, stronger and healthier than before.
With female athletes much of the management is very similar to that for any patient. However in some cases the following professionals need to be consulted to ensure the proper course is charted: a GP or sports physician; general or sports psychologist; and dietitian.
If you’ve suffered a thoracic crush fracture or have osteoporosis and would like help to develop a rehab program aimed at preserving bone mass come and see one of our highly qualified physios today [ Click here to Request an Appointment ]
Costovertebral (CVJ) Sprain
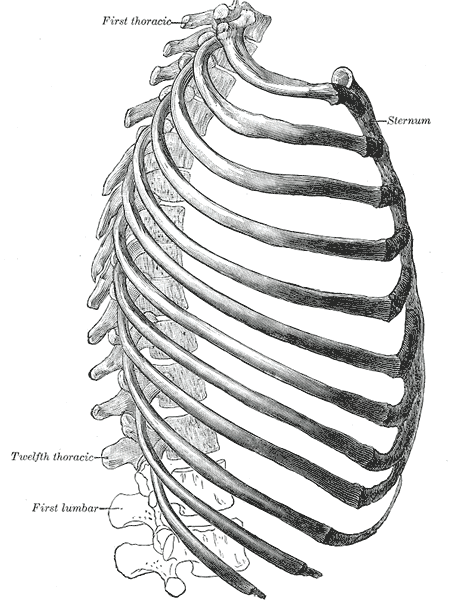
Our aptly named ribcage acts to protect our heart and lungs, serves as a framework for our torso and an attachment point for the muscles and the connective tissues of respiration and those that stabilise and move our upper body, shoulders and neck. The ribs attach to each vertebra of the thoracic spine at the costovertebral joints.
A sprain of the costovertebral joint may include damage to the ligaments, cartilage or joint capsule.
Risk Factors / Causes:
CVJ sprains occur in response to acute injury usually involving sudden twisting, bending or hyperextension; prolonged poor postures; and repetitive tasks.
We’ve seen CVJ sprains in underground coal-miners who perform repetitive overhead lifting; in football players who’ve been tackled awkwardly; in gym goers who’ve lifted weights that are too heavy; and in office workers who sit for prolonged periods with a fixed and flexed thoracic spine.
Management:
Good management starts immediately at the time of injury with the ever reliable rest (R), ice (I), compression (C), and elevation (E). Get this part right and your recovery time can be dramatically reduced.
Physiotherapy treatment to reduce inflammation and manage pain starts early on and as recovery progresses the physiotherapist works with the patient to reduce muscle spasm, restore tendon and muscle strength and regain joint range of motion.
We then work to address factors contributing to the original injury including poor biomechanics; restricted neural tissue; poor lifting and manual handling technique; inadequate core strength; and suboptimal cardiovascular fitness.
The last, and often overlooked, component of rehab is sport, work or lifestyle-specific retraining. If your job has you lifting, pushing or pulling heavy loads; you sit in front of a computer all day; or you play in the NRL and need to regain full explosive power – whichever it might be we work with you to return you to your full pre-injury level of function.
Think you’ve sustained a CVJ sprain or need help with your post-injury rehab come and see one of our highly qualified physios today [ Click here to Request an Appointment ]
Chronic
Scheuermann’s Disease
Scheuermann’s Disease is a developmental disorder affecting the thoracic and to a lesser extent the lumbar spine. The disease is characterised by wedge-shaped vertebral bodies (the solid roundish part of the vertebra) and irregularities in the interface between the intervertebral disc and the bone, known as Schmorl’s Nodes. Wedging of the vertebral body occurs due to asymmetrical growth of the bone, with the front growing either abnormally or at a slower rate than back.
Sufferers of Scheuermann’s Disease will often present with a stiff, rounded or kyphotic and painful thoracic spine. Extension will be limited and combined rotation extension movements such as a tennis serve will be painful.
Patients will often present to us with conditions resulting from extra stress placed on adjacent tissues due to the loss of normal joint range associated with Scheuermann’s Disease. These may include costovertebral joint sprains; headaches; rotator cuff degeneration; or thoracic outlet syndrome.
Risk Factors / Causes:
In short no one really knows why Scheuermann’s Disease occurs. There is believed to be a genetic component and it would appear to be more common in males but more than that we don’t really know.
Management:
Physiotherapy treatment to reduce inflammation and manage pain starts early on and as recovery progresses the physiotherapist works with the patient to reduce muscle spasm, restore muscle strength and regain as much joint range of motion as is possible.
We then work to address aggravating factors including poor biomechanics; restricted neural tissue; poor lifting and manual handling technique; inadequate core strength; and suboptimal cardiovascular fitness.
When Scheuermann’s is a “driver” for a condition such as a rotator cuff tear (insert hyperlink) we make sure that the rehab process manages the shoulder but also addresses the thoracic mobility and strength issues that played a role in the development of shoulder pain.
The last, and often overlooked, component of rehab is sport, work or lifestyle-specific retraining. If your job has you lifting, pushing or pulling heavy loads; you sit in front of a computer all day; or you play in the NRL and need to regain full explosive power – whichever it might be we work with you to return you to your full pre-injury level of function.
Think you suffer from Scheuermann’s Disease or need help with your post-injury rehab come and see one of our highly qualified physios today [ Click here to Request an Appointment ]
Thoracic Outlet Syndrome
The thoracic outlet is a region of the shoulder and neck through which exit various nerves and blood vessels on their way down the arm. Compression or restriction of these nerves and vessels can lead to a variety of symptoms in the arm including a sensation of heaviness, weakness, numbness, ‘pins and needles’ and pain.
Risk Factors / Causes:
The thoracic outlet is bounded by the scalene muscles of the neck, the clavicle (collarbone) and first rib and a bony projection of the shoulder blade known as the coracoid process. Damage to the bony structures; restriction or inflammation of the muscular components; repetitive overhead work; poorly fitting or poorly designed bras; and poor posture can all lead to compression or restriction of the subclavian artery, the subclavian vein or the nerves of the brachial plexus giving rise to thoracic outlet syndrome symptoms.
Management:
In most cases we aim to conservatively manage the painful symptoms and work on regaining range of movement, strength and movement control. In physio-world the way in which the shoulder blade and arm move together is referred to as scapulohumeral rhythm. Restoration of normal rhythm whilst maintaining scapular stability, particularly at the extremes of range, is essential in achieving pain-free movement. Improving posture and increasing range of movement in the joints of the neck, thoracic spine and ribcage plays a big role in managing this condition.
Once we get the basics under control it’s time to challenge the patient with higher level sport and work-related tasks such as lifting, pushing and pulling under load and at speed.
If you think you’re suffering from thoracic outlet syndrome then contact us and come and see one of our highly qualified physios today [ Click here to Request an Appointment ]