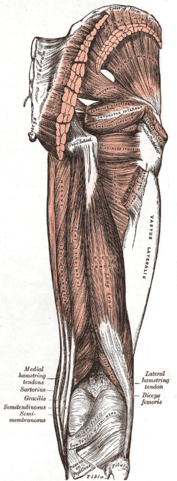
Even the most non-sporting amongst us are familiar with the “hammy” strain. “Pulling a hammy” involves tearing one or more of the four muscles at the back of the thigh.
Risk Factors / Causes
When we run, the hamstring is called upon to shorten (i.e. pulling the heel towards the bottom – referred to as a concentric contraction) and then lengthen in repeated high-speed cycles. During the lengthening phase it must perform the difficult task of contracting whilst lengthening to stop the lower leg from simply flicking out – we refer to this contraction/lengthening process as an eccentric contraction. Whilst the contributing factors vary, it is a loss of coordination between concentric and eccentric functioning that is at the basis of most hamstring injuries. Some of the contributing factors include: fatigue; inadequate warm-up; pre-existing injury and a history of lumbar spine dysfunction or injury.
Management
Hamstring injuries are a source of immense frustration for an untold number of athletes. They can be recurrent, debilitating and difficult to rehabilitate particularly where there is an existing history of injury and / or a contribution from the lumbar spine. Age-related changes in the lumbar spine are one of the reasons why the older athlete is particularly at risk of hamstring injury. This is why effective early management of a hamstring strain is so important.
The first step is to control the extent of injury through rest/ice/compression and elevation (RICE) and the often neglected, avoidance of alcohol and other aggravating factors.
Physiotherapy treatment will focus upon restoration of muscle length, muscle strength, endurance and coordination. This occurs in conjunction with assessment and treatment/management of lumbar spine pathology and the associated restrictions in mobility and function of the nerve tissue (sciatic nerve) as it exits the back and makes its way through the buttocks and back of the leg.
As the patient progresses treatment begins to address sports-specific factors such as running technique and lower limb biomechanics. In many cases ongoing management through Pilates, stretching, strengthening and hands-on physio keeps the athlete on track
Think you’ve strained your hamstring or need help to stop it happening again then come and see one of our highly qualified physios today [ Click here to Request an Appointment ]
Corked Thigh
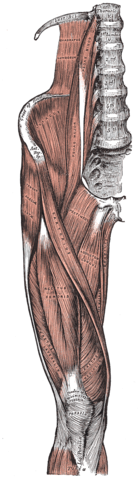
A corked thigh – Charlie Horse to the Yanks out there; corky to the Victorians – is damage to the thigh muscle resulting from a direct high-velocity impact.
Risk Factors / Causes:
A corked thigh is common during impact sports when a knee or similar body part impacts the thigh of an opponent. The impact leads to significant tissue damage and bleeding within and between muscles.
Damage confined within a muscle (intramuscular) can lead to significant loss of function and pain and can prevent an athlete from running for weeks. Poor recovery from an intramuscular cork may lead to a condition known as myositis ossificans where bone is formed within the muscle.
Damage that leads to tearing of a muscle and its surrounding connective tissue (intermuscular) will have significant bleeding initially but a quicker recovery.
Management:
Good management starts immediately at the time of injury with the ever reliable rest (R), ice (I), compression (C), and elevation (E). Get this part right and your recovery time can be dramatically reduced.
The direction of therapy is dictated by whether the injury is predominantly inter- or intramuscular. Recovery is typically slower with an intramuscular injury and aggressive early treatment can in fact lead to delays in return to sport, so a thorough assessment is critical.
Physiotherapy treatment to reduce inflammation and manage pain starts early on and as recovery progresses the physiotherapist works with the patient to restore muscle length, restore tendon and muscle strength and regain joint range of motion.
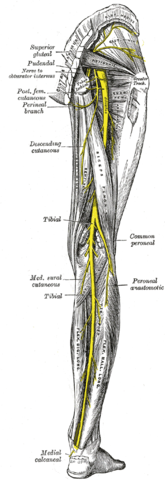
Sciatica is the term used to refer to pain felt along the pathway of the sciatic nerve as it exits the spine and makes its way through the buttocks and down the back of the leg. It’s worth remembering that not all pain felt in the back of the leg is sciatica, even if the cause of that pain is an injury to the back. It’s also worth remembering that not all sciatica sufferers experience their symptoms as pain. For some it’s burning, tingling or numbness. These symptoms may be felt on their own, may occur in addition to pain and may also be associated with muscle weakness in the effected limb. We’ve listed this in the chronic section although in some people it will start with an acute episode. If not well managed in the acute phase it will over time become a chronic condition.
Risk Factors / Causes
True sciatica arises from irritation of the sciatic nerve due to a bulging lumbar disc or similar conditions that cause compression or chemical irritation of the nerve and its sheath.
Significant trauma to a lower lumbar disc or other spinal structures may lead to sciatica; however it is just as likely to occur as a result of degenerative changes occurring over time.
The incidence of sciatica tends to peak between the ages of 30 and 65 coinciding with a time in life where degenerative changes in the spine become more apparent and people become more sedentary. After 65 the spine tends to become stiffer yet more stable so complaints of sciatica decline.
Management:
It’s important to remember that sciatica is a symptom – the real focus of our physio treatment is to isolate the underlying cause and treat that.
Patients presenting with sciatica often are in a lot of pain, so we use techniques to reduce muscle spasm, support posture and reinforce pain-relieving movement patterns.
In addition to pain-management we look to restoring optimal joint movement; normalising muscle recruitment patterns; and enhancing core stability. All of these techniques are gradually progressed until we are replicating the loads that would be experienced in a work, leisure or sport environment. Many of our patients with sciatica respond well to Pilates-based exercise to improve their muscle strength and endurance and general joint and body mobility.
In some cases surgery is required to address the underlying cause of the sciatic symptoms. This may be a stabilisation procedure; a discectomy or micro-discectomy: a procedure to remove herniated disc tissue impacting upon the nerve root; or even a disc replacement. Once the surgery has been performed we begin a process of rehabilitation that is very similar to what we undertake for the non-surgical patient: that is focusing on pain-management; re-education of movement patterns; improved core control; muscle strengthening and endurance training; and a return to full normal function.
If you’re suffering from sciatica or would like to start a Pilates-based rehab program to prevent a reoccurrence of sciatica then come and see one of our highly qualified physios today [ Click here to Request an Appointment ]