To get an idea of what your shoulder does take your right hand and try the following: scratch your nose; scratch your left bum cheek; scratch your belly; give a high-five; do your best karate kid impression and wax on wax off; pull a curtain across from left to right and right to left; take your hand up behind your back with the palm facing out; take your hand down behind your head with the palm facing in. Your shoulder must accommodate this huge range of movement safely, smoothly and whilst remaining stable. It’s the potential conflict between mobility and stability that contributes to some of the shoulder impingement issues that you can read about here.
Risk factors / Causes:
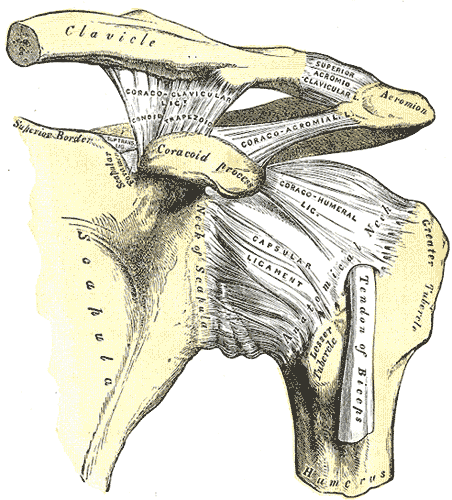
The most common cause of shoulder dislocation occurs when the arm is held away from the body during a fall or tackle. We physios refer to this vulnerable position as the stop sign position – arm at 90 degrees to the body, hand and palm facing forwards. The arm is forced backwards and the trunk forwards resulting in the shoulder popping out of its socket. The first time shoulder dislocation typically causes widespread damage to the bony, muscle and connective tissue of the joint (the glenohumeral joint).
Occasionally we see patients who have had multiple dislocations resulting in an unstable shoulder that can pop in and out (sublux) with little or no pain or loss of function. This type of instability can also occur due to repetitive stress of the joint as seen in swimmers, golfers and volleyballers. It is also evident in people with genetically hypermobile joints.
Management:
The rehabilitation options for a dislocated shoulder are similar to those for the ACL. If you’re a footballer, a surfer a gymnast or bricklayer reliant upon a stable joint throughout the entire range of movement then off to the surgeon you go. Even if you’re none of these, surgery may be required to deal with the painful symptoms emanating from the widespread tissue damage often seen post dislocation.
Irrespective of the management pathway the primary goals are to restore range, stability and higher-level sport or work-specific functioning.
Our arms and legs are often referred to as appendages and unfortunately this is how many shoulder rehab plans are designed, forgetting that the arm and shoulder function in conjunction with the joints, muscles, fascia and connective tissue of the chest, back, butt and legs. Here at Construct Health we rehabilitate the entire body, stabilising the shoulder in conjunction with reconnecting and re-establishing its dynamic relationship with the entire body.
If you’re goal is to rebuild a dynamic highly functioning shoulder after dislocation then contact us and come and see one of our highly qualified physios today [ Click here to Request an Appointment ]